A comorbidity is a separate disease process that might not kill a person, in and of itself, but combined with other comorbidities, might overwhelm the body’s ability to compensate, and kill the patient. Usually, comorbidity refers to sicknesses. For example, a lung cancer patient who also has cirrhosis of the liver.
In the TacMed world, we sometimes use comorbidity to refer to external, traumatic, or self-inflicted contributing factors. The tragic case of George Floyd had a series of comorbidities we can use to increase our understanding, so we can prevent or at least reduce similar incidents in the future.
George Floyd experienced a panic attack when he realized that his own behavior (passing counterfeit bills while taking drugs on probation) was going to land him back in jail. He told the officers he was claustrophobic and afraid of getting COVID-19 if he want back to jail.
I get it.
I, too, am claustrophobic. I used to HATE when those metal doors locked shut behind me, when I went to jails and prisons to interview suspects. Sometimes, it was all I could to, to appear calm and collected during interviews–and I knew I would be able to leave when we finished. I spent about 3 1/2 days in something very similar to a POW camp once, and I wouldn’t wish jail or prison on my worst enemy. But I put people in prison, because they had waived their right to freedom by victimizing others.
Jesus once faced scribes and pharisees who wanted him to condemn a woman they caught in adultery. He said “let he among you who is without sin be the first to cast a stone at her.” Indeed, as more and more of life passes behind me, I find myself growing ever less eager to throw stones at others. There are professionals in our society who carry the responsibilities to investigate, charge, judge and sentence. I gladly leave the burdens of condemnation to them.
–Major Forrest E. Morgan, Living the Martial Way
Many criticized the “tent city” jail Maricopa County set up to alleviate overcrowding in their brick and mortar lockup. But being claustrophobic like my tocayo George Floyd, I’d rather be there, breathing the outdoor air, even at 100+ degrees in Arizona, than in air conditioning behind a locked metal door.
Maricopa County’s outdoor jail in the sweltering Arizona desert. No, wait–that was my quarters in the sweltering Arabian desert.
Perhaps one day we’ll find a less inhumane way to correct lawless behavior and to protect our citizenry from being victimized by the lawless. But for now, claustrophobia is not, and cannot, be a get out of jail free card.
Floyd was repeating “I can’t breathe,” over and over. He even said it before police tried to put him in a patrol vehicle (watch the whole video, not just the tragic last nine and a half minutes). Although the causes of a panic attack are psychosomatic (all in one’s head), the effects of a panic attack, including a rapid, strong heartbeat, and shortness of breath, can be very real.
Floyd was never actively resisting. Witnesses and pundits interpreted this to mean he did not resist at all. There are two types of resistance to arrest:
Active–striking or taking a swing at the officers. Floyd did NOT do this.
Passive–not cooperating. Think environmental activists lying down in front of a bulldozer.
Floyd resisted passively, by not just sitting in the police SUV and letting them take him to jail. After Floyd pushed his way out the other side of the SUV they tried to sit him in, the officers were duty-bound to prevent his escape in some way. How they did it is the crux of this article.
Contrary to apparently popular belief, if a suspect doesn’t want to go to jail, the cops do NOT have the option of saying “Wow, I had no idea you felt so strongly about this. Our bad. Have a great life. Let’s go get a doughnut,” and just walking away. If they had let Floyd run into traffic and he’d gotten hit by a car, they would have been held responsible.
Their dilemma: George Floyd did not want to go back to jail. It was giving him a panic attack. Floyd was a huge, very muscular guy. He was six feet, four inches, and 220+ pounds of solid muscle. Floyd had done time for several crimes, including aggravated robbery with a deadly weapon. After getting out of jail most recently he had, by all accounts, mostly turned his life around. He worked as a bouncer at different clubs, including one where the officer who later knelt on his neck worked an off-duty security gig.
As a former law enforcement Defensive Tactics and Use of Force instructor, I’ve often wondered what was going through that officer’s mind, kneeling on George Floyd’s neck even after Floyd stopped being vocal. This is pure speculation, but perhaps the officer had seen what Floyd was capable of when he worked as a bouncer. I still can’t wrap my brain around the duration of the officer’s control technique, when he could have switched his team to medical rescue mode much sooner.
Friends described Floyd as a “gentle giant.” But if he chose not to be gentile, on his feet, he could have taken several of the cops if he’d wanted to. Long and oft-bitter experience in law enforcement shows that a suspect who does not want to go back to jail may fight. They can suddenly change from pitiful to raging maniac, and often do.
Having heard Floyd say he couldn’t breathe since they first tried to apprehend him, the officers realized it wasn’t just a temporary thing. He was, indeed, experiencing a physiological emergency. They pinned him to the ground to keep him from fleeing and called for an ambulance, which wound up taking nine minutes to get there.
Why on the Ground?
My first three years with the feds, I was in the Border Patrol in southmost Texas. As a rookie agent, one of the first times I caught a group of aliens who had run from us, I had them standing around when my training officer caught up with us. After we got them in the back of our rig, he took me aside. “I didn’t like what I saw when I got here, partner,” he said. The tone he used was that of a parent saying “I’m not angry, I’m disappointed.” He went on to explain that we would almost always be outnumbered by the people we apprehend. If I had them sit down, or even lie down, gravity would be on my side. That way, if they choose to gang up on me, it would take them a second to get back up, which would buy me time to react.
In the agencies I worked for, all potentially combative suspects went to the ground to be cuffed and searched. Image from refresher training we did on Felony Car Stops
Steve Wheeler, officer survival instructor for CPD, told us newbies that “All combative suspects go to the ground.” That way your partner isn’t trying to put him against a wall while you’re trying to lean him across the hood and your backup is trying to put him on the ground. The ground is a good place to standardize, again because of gravity.
Steve Wheeler, expert on officer survival. Image on display at CPD HQ
The MPD officers restrained George Floyd the same way I was trained to restrain larger suspects who were resisting, passively or actively–horizontally, with my weight on their neck, shoulder, or back. I restrained resisting suspects that way, in accordance with my training and agency policies, throughout my law enforcement career, without killing any of them. Far more often than actually restraining resisting subjects, we restrained each other that way in periodic refresher training (see Prone Stabilization below). None of us died from it.
Internal and External Comorbidities
Here is where Floyd’s comorbidities kicked in. Especially, his “severe underlying heart disease:” blocked coronary arteries that had enlarged his heart (a sign of impending heart attack).
Additional external comorbidities included:
Floyd had put fentanyl and methamphetamine into his system. I understand it was enough to kill a non-user who had not built up a resistance by abusing both substances over a long period of time, but I don’t know that for sure.
Floyd’s head (and hence, his airway) was near the exhaust of the cruiser he had crawled out of. Car exhaust is bad for you. People often use it to kill themselves. That comorbidity could easily have been negated by turning off the engine–far easier than it would have been to move him, since Floyd was a large man. As far as I know, none of the cops turned off the engine. Once while serving a warrant on an “extended stay” hotel room that was very, very dusty inside, my fellow agents tossed in a flash-bang distraction device. As the tactical medic on scene, I got called up because one of the residents was having difficulty breathing. I was able to solve the problem by simply removing her from that heavy-particulate environment and into the fresh air outside.
The position of Floyd’s neck and the pressure placed upon it may have restricted the blood flow through half of Floyd’s carotid and jugular vessels (see mata leão below).
The police put Floyd in a prone position, i.e., on his belly. The face-down position has been known, since at least the 1990s and probably earlier, to cause positional asphyxia. Floyd had huge shoulders and arms, but his belly was relatively flat. Positional asphyxia is more of a problem for round-bellied people like me. But the weight of an officer on his neck and (especially) another on his torso contributed to his positional asphyxia.
It’s OK to prone a suspect out; just don’t leave them there forever, ESPECIALLY if they are experiencing a physiological emergency.
It was very likely the combination of all of the above factors, those comorbidities, that killed George Floyd.
Airway issues
It’s clear that the weight of the officer on Floyd’s neck did NOT block his airway. We know this because Floyd kept speaking for some time. If you can say “I can’t breathe,” you MUST have an airway. The ONLY way to talk is to pass air through the vocal cords in your neck. I’m not trying to “gaslight” anyone here. It’s a physiological fact. It works the same on all human beings, whether their skin is black, brown, red, white, or yellow.
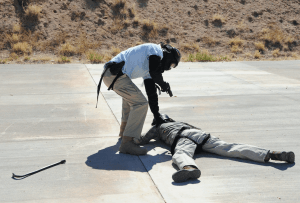
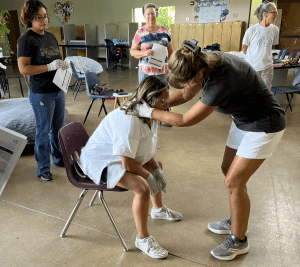
This photo was taken during a Public Safety Integration / Tactical Emergency Casualty Care course we put on for first responders at Ft Huachuca, AZ. The soldier in the black t-shirt volunteered to be a “victim” role player. In this scenario, he had been shot in the side of the neck, and was bleeding profusely. The role player is applying direct pressure to his own “wound.” The responding officer is applying even more direct pressure to his neck, directly over the victim’s hands (as we trained them), while getting ready to apply the pressure dressing in his left hand. The victim role player was young and healthy and was able to breathe the whole time.
Looping under the opposite arm, you can apply a pressure dressing to the side of the neck without choking the patient.
Recall that in the MARCH algorithm, A is for Airway and R is for Respirations. It is possible to have an airway and still have difficulty breathing. Pundits on both sides of the larger debate about reforming the way the law is enforced conflate the two of these as the same thing. They are not. In George Floyd’s case, even though the officer on his neck clearly did not block his airway, the officer(s) on his body were making it harder for him to breathe.
Pressure applied directly to the front of the throat and can crush the windpipe. We know this didn’t happen to Floyd because George kept saying “I can’t breathe.”
The Mata Leão
It is quite possible to kill a man by applying pressure to either side of the front of his neck at the same time.
Brazilian Jiu-Jitsu practitioners frequently use a submission hold called the rear naked choke, or “mata leão.” The person applying the choke squeezes both front sides of the neck between their forearm and biceps, reducing the circulation in the carotid arteries. They use this submission hold till their opponent taps out or passes out.
Setting up the mata leão. Next she’ll slide her left hand behind the head and apply forward pressure to it, forcing the carotids into the V between her forearm and her biceps.
“Mata leão” is one of the classic submission holds of Brazilian Jiu-Jitsu. In a real fight it represents one of the safest and most effective means of controlling and subduing a powerful attacker. In the heat of real combat a strong-willed or intoxicated attacker can endure tremendous pain and still press home his attack. However, no matter how strong-willed or intoxicated he is, if a “mata leão” is well applied, the fight is over.
. . . Should you render an attacker unconscious, release the hold and lay him down on his side. He will come back to consciousness by himself.
–John Danaher
Hold a mata leão too long, though, and the person you are choking will die.
They taught us the rear naked choke at all three of my police academies (military, state, and federal). It is still a viable life-saving tool in deadly force situations, although due to its deadly potential many jurisdictions have removed it from the list of “authorized” custody and control techniques.
Such blanket prohibitions are well-intended but stupid. If someone is going to die if I don’t stop the bad guy, I will use whatever means are necessary to stop them–whether that’s choking them till they pass out (which they would probably prefer) or shooting them, or stabbing them in the eye with a Leatherman tool if I need to–and you can give me days on the beach or fire me or sue me afterward, because I or my partner or some innocent victim or perhaps all of us will still be alive. But if the rear naked choke is prohibited by law, even in deadly force situations, an officer could go to jail for using it to save lives–perhaps even the suspect’s life. The faqct that well meaning but ignorant peole are passing such laws these days is one of many reasons why departments can no longer fill their authorized patrol positions. And no, thowing money at the problem won’t fix that. Nobody wants to be put in a positon where they might be incarcerated for trying to live till the end of their shift.
This is a good place to reiterate that George Floyd did NOT constitute a deadly force threat. He wasn’t trying to kill anybody. He just didn’t want to go to jail.
It’s possible that the pressure the lead officer was putting between Floyd’s shoulder blades might have reduced the circulation in one of Floyd’s carotids or the other, by pressing the side of George’s neck against the pavement. Reducing the blood flow to the brain by 40% or more could very well have been a contributing comorbidity.
But it cannot, all by itself, have been the only cause of death. The only way for a mata leão to kill someone, or to work at all, is to apply pressure to both carotids simultaneously (see Renzo and Royler Gracie’s Brazilian Jiu-Jitsu: Theory and Technique, pp. 120 – 21).
You can press hard with a thumb on one of your carotid pulse points, in the valley off to the side of your Adam’s apple, between it and your sternocleidomastoid, the muscle running from behind your ear to the medial, or inside, end of your collar bone. After a short time one of your eyes will start to grey out, but the other eye will still be working.
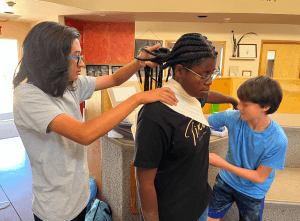
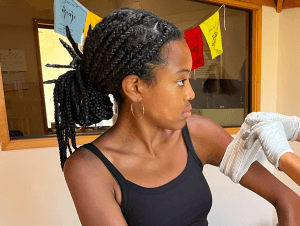
This young lady’s right sternocleidomastoid is clearly visible in this photo. It runs from behind her ear to the inside end of her collar bone. Her right carotid pulse point lies in the triangular valley to the right of that, below her jaw, between the sternocleidomastoid and her trachea, or windpipe.
Our body is marvelously made, with multiple redundant safeguards. We have two kidneys, two lungs, two eyes, two carotids, two of other things for a reason.
What did the medical examiners say?
At trial, one medical examiner, Dr. Lindsey Thomas, testified she believed Floyd died of positional asphyxia. Dr. Andrew Baker, who had been trained by Dr. Thomas and signed Floyd’s death certificate, stated that he believed Floyd died of a heart attack. Technically, we all die of a heart attack, since we list TOD (time of death) as the moment the heart stopped. How could two medical examiners with very similar training arrive at different conclusions?
Really, they did not. Both agreed it was a combination of factors–in other words, comorbidities–that killed George Floyd. But the death certificate only has one block for Cause of Death, so Dr Baker had to go with his best educated guess as to which of those several causes was figuratively the most important nail in the coffin.
I did not follow the trials (the info above is from a media summary, which can be problematic–see grey box below), but it’s likely the prosecutor or defense attorney who pressed them for a cause of death on the stand wanted the medical examiner being examined (or cross-examined) to simplify it to one most important cause for the jury. I can almost hear them saying something like “Yes, yes, but if you had to boil it down to the most important factor in his death, which would it be?” Depending on whose side the trial attorney was on, they wanted to hear whichever uttered word was more likely to convict or exonerate the cops on trial.
Trial attorneys get paid to do things like that. They are not supposed to ask leading questions. So instead they demand a yes or no or oversimplified responses to questions which can only have complex answers.
I once gave a deposition (pre-recorded testimony) in a trial about a police gun battle in which the murder suspect had been into his third 30-round magazine before he went down, and the multiple police officers who returned fire were well into triple digits of rounds fired back. The deputy closest to me when the smoke cleared had shot 44 rounds himself. I only knew this because he started with 46, and told me, as we crouched behind a Caprice with one suspect down and two more still at large, that he was down to two rounds.
I tried to loan him one of my magazines. Despite being in different agencies, he and I had the same make of pistol–we both had Berettas–but alas, they were in different calibers.
His duty pistol was a Beretta 92, in 9mm. My issued Beretta 96D Centurion looked similar, but shot .40 cal.
There were about a dozen officers involved. The gun battle took place at relatively extended range for most participants (thankfully, in a sparsely populated rural area) and most of the rounds fired by both sides missed. It went on for several minutes, which seems like forever, in a gunfight.
One of the attorneys taking the deposition wanted me to estimate the exact number of rounds fired. Of course that would have been impossible for any witness. So many people were shooting at the same time, I could not have counted the shots if I’d wanted to–and I was not so inclined. Apart from being surprised by the extended duration of the firefight, I was not interested in the number of shots while it was happening. I had far more pressing matters at hand.
When I told the attorney it sounded like it lasted a long time, but I had no idea how many rounds were fired, he insisted that I give him a number. He was not trying to arrive at the truth. He was trying to pin me to a specific answer that could NOT possibly match the physical evidence exactly (except my mere chance), so later on in the trial, if my testimony went against his client’s case, he could use that mismatch to refute my testimony. Pretty simple trick they learn on something like day three of Depositions 101 in law school.
I refused to take the bait and said I couldn’t possibly know for sure, but that if he really wanted the answer, he could count the empty cartridge casings found by the investigators afterward (both sides had access to those investigative reports, of course). He relented and moved on to a different line of questioning. He might have pressed the issue if it was later on in the trial, my testimony was critical, and a jury was watching.
Similarly, the news media does not have the bandwidth, the airtime, or the print space for a complete examination of the facts. They cannot give you all the available information so they, too, dumb it down to single words. This can end up being disingenuous, which in this context means truth so oversimplified it becomes a lie.
For example, if a guy named Smith is stabbing you to death, so you shoot him to death before he finishes the job, sooner or later (perhaps while you are still in the hospital) you will read about your case that the “Medical examiner rules Smith death a homicide.” Well, of course it was a homicide. He died from too much lead, not too much linguini. The fact that it was a justifiable homicide may not make it into the 20 second sound byte. I would go so far as to say it probably won’t.
Their readers or viewers, many of whom have the attention span of a carrot, will more often than not infer a lie–that it was your fault–from that statement, because the media told them an oversimplified version of the truth. The word “homicide” implies it was a murder (well, it was, of sorts) without explaining the reasons why. The vast majority of the public will not read down to paragraph eight where the reporters may or may not bury the fact that the “homicide victim” was stabbing you at the time of his perforation.
Hopefully, none of those readers or viewers will end up on your jury.
Prone Stabilization
When I got into civilian law enforcement, I was trained to restrain combative–or potentially combative–suspects prone, in a few different ways. After performing a rear sit-out takedown, for example, I was to “stabilize” the prone combative suspect thusly:
“As the suspect is spun around, the officer must maintain the grip around the suspect’s middle, forcing the suspect to the ground, face down with the officer landing on the suspect’s back. As soon as the suspect contacts the ground, the officer must release his / her grip and reposition so that he / she is at a right angle to the suspect, and then pin the suspect to the ground. This is accomplished by the officer using his / her forearms to simultaneously push down on the suspect’s neck and lower back.”
–Wheatland PD Self Defense and Suspect Control study guide, technique approved 24 Mar 1993, p. C-11.1
With that technique, I essentially planked, with my elbows on their neck and back, so only about half my weight was on the suspect. The other half was pressing into the ground through the toes of my boots. The feds taught us different techniques, but due to primacy of training I automatically reverted to that method I’d learned in ’94 a decade later, when I tackled a fugitive who was running from a US Marshall’s FIST team.
The primary means of prone stabilization I learned in ’94 was with the knees:
“As soon as the suspect is in the ground, the officer must immediately stabilize the suspect to maintain control and discourage further resistance. The officer must immediately pin the suspect to the ground using his / her weight on top of the suspect. When the officer is working on the suspect’s right arm, the officer’s right knee will be placed on the suspect’s back between the shoulder blades, and the left knee will be placed either on the suspect’s lower back or on the ground beside and touching the suspect’s ribs. [This was similar to the “baseball catcher’s” method for cuffing we learned later at FLETC, the Federal Law Enforcement Training Center; it was reversed (a mirror image) for the left arm.] . . . If the suspect is still resistive, the first knee may be placed on the neck area in order to pin the head down, but care must be taken by the officer not to drop full speed with his / her weight onto the neck.”
–Wheatland PD Self Defense and Suspect Control study guide, technique approved 01 Oct 1990, p. C-5.1
Later in my career when I was a special agent, the National Firearms and Tactical Training Unit (NFTTU) of my agency actually paid a champion cage fighter as a consultant. They would try different techniques to restrain him, and he would escape from them.
Eventually, based on the cage fighter’s input, we changed our prone cuffing technique. We pivoted 90 degrees from the catcher’s position, moving the pressure of our shin and knee from between the shoulder blades to on one shoulder blade adjacent to the neck, to avoid damaging the suspect’s cervical spine and / or trachea (as far as I know, neither of those two were listed as damaged during either of Floyd’s autopsies). Combining the weight of one’s shin on the shoulder with an arm restraint was the one position that cage fighter could not escape from, so my agency adopted it.
I said this before, but it bears repeating here. Throughout my career, I knelt on the neck, or between the shoulder blades, or the shoulder very close to the neck, of many friends and fellow cops when learning, practicing, and later teaching arrest techniques. They did it to me too–over, and over, and over, especially in Defensive Tactics Instructor (DTI) schools. After serving as a DTI, I went back to our NFTTU to teach other DTIs. It didn’t kill or injure any of us. None of the suspects I did that to died.
Much has been made of the fact that the officer in charge had one or possibly even both toes off the ground placing almost all of his weight on Floyd. In my experience, how much weight you can get on the suspect depends in large part on how thick they are from fore to aft. It is possible to apply the same “catcher’s position” to different suspects, with one appearing to rock most of your weight onto your heels (because the “hill” of their shoulder is so steep) and the other where more of your weight is on the suspect because they are skinny and flat fore to aft like a pancake.
If, because they are flailing around or fighting back (Floyd was NOT doing either), you feel like you must get more of your weight on the suspect to control them, you will have to compensate by shifting more of your weight onto the suspect somehow. As someone with short, stubby legs, I often struggled with this when the training partner I was restraining was thick from fore to aft, as Floyd was. I compensated for my stubby legs with thick suspects by reverting to the planked position I learned in the early ’90s. That at least got most of my weight–the weight of my upper body–on the subject and I was less prone to be bucked off than if I was in a catcher’s position.
Questions about Floyd’s Tragic Death
Would George Floyd have died that day if the officers hadn’t tried to arrest him?
Probably not. But only probably.
Would George Floyd have died that day if he didn’t have a preexisting heart condition?
Almost certainly not.
Would George Floyd have ODed that day if they had not tried to arrest him?
Probably not, but we’ll never know.
All we know for sure is that George Floyd is, in fact, dead.
The combination of all those comorbidities and external factors did George Floyd in. To believe otherwise is to be blinded to reason by understandable anger.
The officers who attempted to arrest Floyd had zero control over Floyd’s internal comorbidities (heart disease, fentanyl / meth, panic attack), nor over Floyd’s criminal behaviors which brought them to the scene in the first place. But they had absolute control over at least two external comorbidities: keeping his face near the exhaust of a running engine, and how they restrained him. That’s why the officer who was in charge is in jail today. The other officers who restrained Floyd are in jail because they followed the chain of command.
“I was only following orders” did not help the Nazi war criminals on trial at Nuremburg. But it would be disingenuous of me–something I frown upon the media being–to go any farther with that comparison, because the two injustices are orders of magnitude apart. Joe Stalin, someone we should NOT be trying to emulate, said that one man’s death is a tragedy, but a million deaths is a statistic. Both can be unjust.
One officer went to jail because he happened to be nearby. He was facing the other way, maintaining the peace by keeping the crowd away–which was his job, and something I did on many occasions. I was not on that jury, but the sad, honest truth is probably that he is rotting in jail because the jurors were afraid that bad things would happen in their neighborhoods if they did not convict him. If they had exonerated that officer, their family might get death threats, and their town might burn to the ground like Ferguson Missouri had.
In this acrimonious, separatist age, when reasonable, intelligent people on both sides of America’s culture wars are being silenced to avoid offending ignorant, bigoted people (the notion that only one category of people can be bigots is the very definition of bigotry), I could get doxed or trolled or even fatuously accused of racism for stating these truths, based on my long experience and relative expertise in both the medical and law enforcement fields. But I will speak the truth the way I see it.
I’m no expert on anything, and I was no Eliot Ness, but I have arrested people who did not want to be in cuffs and did not want to go to jail. There is no pretty, polite, easy, politically correct, un-hurtful way to do it that looks great on a smartphone camera.
What I could do, though, and did when I could, was to treat them like human beings AFTER I got them under control.
How Can We Prevent Another George Floyd Type Death?
Sitting Up in Leg Restraints
Before George Floyd passed out, they could have sat him up, which would have taken pressure off his lungs.
If I had a suspect / patient who said he could not breathe, and who’s breathing was slowing down, I might very well have sat him up to get pressure off his chest. Many people who are having difficulty breathing prefer to sit up with their elbows on their knees, leaning slightly forward, in what is called the “tripod” position.
People having difficulty breathing often breathe easier if they are sitting up, leaning forward in the tripod position
While it’s almost never advisable to handcuff a suspect in front, they still could have sat George Floyd up.
If I was concerned my suspect patient might try to escape, I could have snapped leg irons on his ankles, to keep him from running away. I’m pretty sure they have leg irons–a short stretch of chain between two ankle-sized cuffs, that prevents spreading the legs far enough to run–in Minneapolis. If Floyd had been combative, that might not have been an option, but he never lashed out at the officers.
The Recovery Position
As soon as Floyd STOPPED saying he could not breathe, probably sooner, those officers should have at least rolled Floyd into a side-lying recovery position to protect his airway (a junior officer even suggested that, but the officer in charge of the scene decided not to and overruled him).
First Aid student checking the back for injuries after rolling the (simulated) patient into the side-lying recovery position. Note that the upper elbow and knee are both down like the kick-stand of a bike, so she stays on the side, keeping pressure off her chest and stomach.
They also should have been checking Floyd’s pulses or for other signs of circulation sooner. It became apparent to most observers that Floyd was unresponsive about six minutes into the restraint (3 minutes before the ambulance got there).
Every officer should have training for gunshot wounds, and most do, but they should also have much more comprehensive medical training. Officers are often the only ones available to perform first aid in tactical situations like that Aurora Colorado movie theater (this can be alleviated to some extent by Rescue Taskforces, a subject for another article).
The sad fact that is relevant here is that most LEOs have inadequate medical training to this day. Many feel (it used to be official policy, and still is, some places), that playing Marcus Welby MD is outside the scope of an officer’s duties and exposes the department to too much liability. But the 1989 Supreme Court case Canton v Harris clearly established that police departments have a duty to train their officers for medical situations which commonly arise in the day-to-day course of their duties.
Forget liability for a movement. Let’s talk about what’s right, and what can ensure that officers and the public they protect can all go home at the end of the day. Many cops feel, correctly, that if they are doing medicine, they will be dropping the ball on their primary responsibilities: protecting the public and their partners.
It’s true that when you are doing CPR or otherwise focused on a patient, you CANNOT watch your own back, or anybody else’s. You will be laser focused on the task at hand.
If this task has your undivided attention, how will you keep bad guys from sneaking up behind you? Don’t abdicate your AOR–area of tactical responsibility–to practice medicine until you have someone assigned to watch your back. For more, see Ways to Fight Tunneling In.
DO NOT APPROACH AND RENDER AID TO A PREVIOUSLY ARMED OR COMBATIVE SUSPECT IF YOU ARE SOLO. But if you have lots of armed friends on-scene, you have that option.
If you don’t render aid to the subject, who will?
I once, quite reluctantly, handed my rifle to a complete stranger (a Cameron County deputy) even though we allegedly still had two homicide suspects at large, because I could not see any suspects, but I could, quite clearly, see my friend Agent Mike Riley urging his partner, Agent Susan Rodriguez, to hang in there as she bled out through her nose and mouth. I felt I was good with a rifle, and only so-so as a medic, but the tactical situation was in hand for the time being, so I switched to medical rescue mode . . . as those Minneapolis cops should have with George Floyd, much sooner than they did.
They had called an ambulance at about the same time they started restraining Floyd. Good for them. But as Floyd began to circle the drain, they should have rolled him onto his side, using a hobble or ankle restraints if they felt he might be faking it so he could escape.
I have taught CPR for the AHA (American Heart Association, through the MTN, Military Training Network), the Red Cross, and the American Safety and Health Institute (ASHI, now called Health and Safety Institute, or HSI). I have certified military, police, and civilians in CPR. I am still a HSI certified instructor.
If you don’t have a mask, don’t forget to pinch the nostrils . . . but that’s a different aspect of airway management than we’re discussing here
Neither of those training and certifying organizations want lay rescuers to spend too much time looking for pulses. If you can’t find a pulse, that’s because their heart has stopped, OR you are looking for a pulse in the wrong place. Don’t do CPR on a person who is talking to you (they can’t do that without a heartbeat) even if you cannot find their pulse. If they stop talking to you, as George Floyd did, look for signs of circulation.
Older medical textbooks, written by white medical providers for other white providers with white patients, say skin that is getting circulation is “warm, pink, and dry.” How to check for circulation on a darker skinned person? Warm and dry still apply. You can look for pink by turning out a lip–if the inside is turning purple, they may be in trouble. Some dark-skinned people have dark pigmentation on the inside of their lips as well, but for most the inside of their lips and eyelids will be pink. You can also press on a palm or nail bed (if they’re not wearing nail polish) to check for capillary refill.
This dark-skinned person’s palm would be lighter if they were not wearing a tourniquet. After pressing on the palm with a thumb, the blanched portion should refill with blood and get more pink–but it does not, due to lack of circulation to the limb
Do not spend a lot of time looking for signs of circulation, or a pulse. If the person isn’t breathing, assume their heart has stopped too, and start CPR.
Earlier CPR could have saved George Floyd’s life.
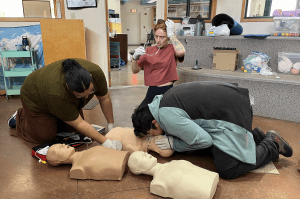
Students practicing CPR. Just about every law enforcement agency requires its officers to be CPR trained–but not all “training” is quality training, or comprehensive training. Sometimes it’s only education, checking a box, and not really trainingh at all.
–George H, 30 year EMT and 7-level military medic
The image at the top of this article is from Yahoo.com.
This article started out as a definition in the Glossary of TacMed Terms. I thought it warranted its own article, with more detailed info, if we are to prevent similar incidents in the future.
Appendix I:
Marker’s Principles of Custody and Control
I re-read these gems for the first time in years while I was refreshing my memory and fact-checking in some of my old Use of Force manuals to write this article.
James Marker, Self-Defense and Suspect Control instructor for the Wheatland Police Department and the Wyoming Law Enforcement Academy, was one of my first civilian Use of Force instructors.
Comparing bruises with my partners after an exhausting but informative session of James Marker’s Custody & Control training
Officer Marker wrote these words before the beating of Rodney King, and decades before George Floyd died. They are still good advice for officers using force and pain compliance techniques today. Items in brackets [ ] were added by me for clarity.
Because your duty is to control the law violator, not to fight him or punish him (these are conflict situations) always apply pain or reasonable force not [to] punish him, but in such a way that the pain alone will let him know what you want him to do.
Be relaxed and alert.
It is not aggression when you take the initiative to confront a law violator.
The Officer’s role in a physical arrest is essentially defensive in nature.
Control of the situation through control of yourself and the suspect.
Arrest is an emotional problem as well as a physical one.
Avoid meeting force with force.
Upon being assaulted, defend or attack the aggression not the aggressor.
Know what you want your subject to do before you apply a control technique.
Apply only the degree of pressure or tension necessary to achieve and maintain control.
Tension / pain vs. Injury.
Be prepared not paranoid.
I think what Principle 4 means is that cops look at arrest dispassionately, as a problem to be resolved. But it’s a very emotional situation for the arrestee, and that can lead suspects to do unreasonable things. Law enforcers should not be surprised by this. They should instead be tactically prepared if the suspect is so emotional about it they would rather kill the officer(s) than go back to jail. And we should perhaps cut the cops a little slack if they get offended, perhaps even mad, when someone tries to take their life rather than owning the inevitable consequences of their criminal actions.
One of the biggest problems facing police officers today is that they are expected to wait until things go south before responding with force. Anyone who has operated on the street knows that coming down hard enough soon enough actually reduces the amount of force the police need to apply in the long run. It saves both police and suspect lives, and prevents more suspect injury than it causes.
That said, it is possible to serve with both caution and compassion. Most cops–the ones you never read about–do.
The principle of pain compliance is that people will avoid pain. For example, hooking a finger in the sternal notch of someone who refuses to sit down, and pushing your fingertip down, will cause most people to avoid the pain by sitting down. If someone who is bowing up on you, getting ready to take a swing, sits down, they are less likely to fight you after they sit down, and less likely to be successful if they do.
Unfortunately, people who are drunk, drugged, or deranged feel less pain are less likely to respond to pain compliance techniques. And they’re the ones most likely to fight.
Principle 3 is often misunderstood, and probably warrants its own article as well. Just remember that the terrorist who blew up the Murrah Building in Oklahoma City, murdering 168 people (including 19 children in a daycare center), was caught because of a “petty” license plate violation. Terrorists, murderers, kidnappers are not caught when we mail them a ticket with a photo from a speed camera. They are often caught when a cop pulls them over, looks a subject in the eye, wonders why the subject’s story doesn’t match what they are observing, and digs a little deeper.
Appendix II:
Marker’s Rules of Custody and Control
Jim Marker wrote these words, too. They have also stood the test of time.
Understand and accept the fact that your objective is control–control of yourself and control of your subject.
You can concentrate on only one thing at a time.
Practice will give the ability to shift your concentration rapidly.
Condition yourself to think problems all the way through [clearly, the officers in Minneapolis did not].
Always know before you apply a control technique exactly what you intend to do.
A man can control his mind only if his mind is relaxed.
Only a flexible mind is capable of avoiding conflict.
Never meet resistance with resistance.
Never use brute strength; instead use the strength and momentum of your subject to your own advantage.
Physical balance and mental balance are equally important.
Use sharp, sudden moves of distraction to short circuit cooperation between your subject’s mind and body.
Use the lag-time resulting from his distraction to your own advantage.
Avoid hesitation, verbal abuse, bluff, unnecessary force and other compensating behavior — it comes from your own uncertainty and lack of confidence.
You can increase your self-confidence by practicing your custody and defense techniques.
Always be ready for the truly peaceful law violator, just as you are always alert to the possibility of violence.