I’m well on my way to becoming what my brother calls a “surly curmudgeon.” Old people like me tend to become set in our ways. We like what we like. Think Danny Glover’s “Sgt Roger Murtaugh” with his S&W Model 19 in (the original movie) Lethal Weapon.
Riggs: “What have you got?”
Murtaugh: “Four-inch Smith”
Riggs: “Six-shooter? A lot of old-timers carry those.”
Skill and experience with any given piece of gear is, to a large extent, the most important determinant of success. It’s far better to be trained and experienced with an older or slightly less capable system than to be mediocre with the latest and greatest. David took a sling to fight Goliath, instead of Saul’s much more capable sword, because he was good with that sling. He knew it well, and probably (if he had wanted to eat while he was out on sheep-watching duty) used it often. It worked for him.
Several different tourniquets work for me. When I was a TacMed, I preferred the SOFTT, Special Operations Forces Tactical Tourniquet (even its earlier, narrower versions) for putting on other people. The SOFTT has always been a sturdy, no-nonsense tourniquet, but it is easier to don if you have two hands to use.
Windlass-tightened tourniquets. L to R: Gen 7 CAT, TMT, older “alligator clip” SOFTT, SOFTT-W.
With tourniquets, wider is better. The SOFTT-W (wide version of the SOFTT) is an improvement over the original, and has a sliding, C-shaped clip (possibly licensed from North American Rescue, who holds the patent on the CAT, Combat Application Tourniquet) to make it easier to apply one-handed.
As a special agent, and on my last wartime deployment, I carried a North American Rescue CAT on me. I still do, because it’s still the easiest I’ve found to apply one-handed. If you are solo and putting it on your opposite arm, you’ll only have one hand to work with.
ICSAVE student applying a CAT one handed
When teaching military and medical professionals how to use tourniquets, we mostly train the CAT, because it is the tourniquet they will most likely find in an IFAK (individual first aid kit, i.e., a “blowout kit”) or a medic’s “jump” bag. As far as I know the CAT is still the tourniquet most commonly issued by the US military.
*****
Enter the RATS
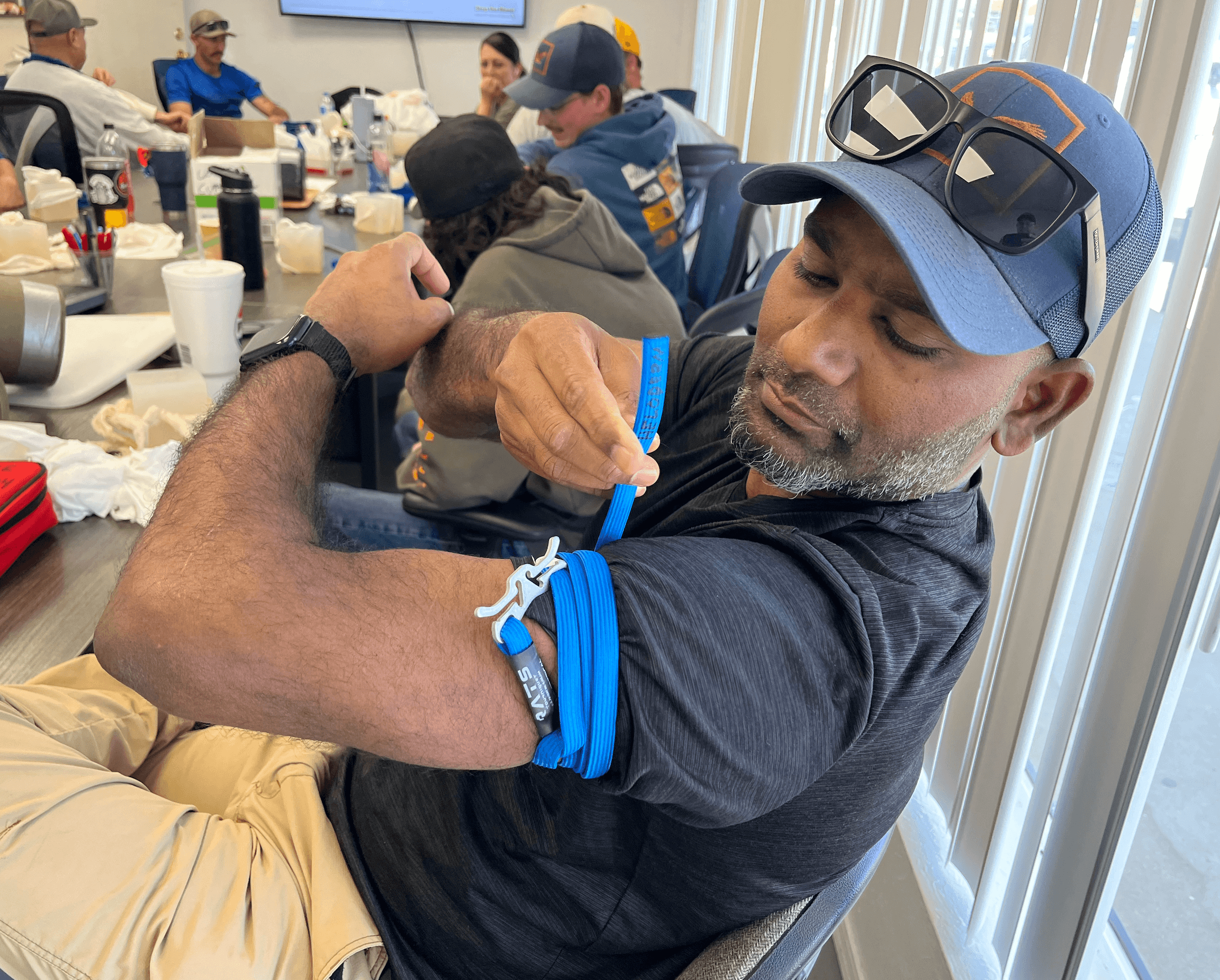
A fellow instructor introduced us to what is essentially a bungee cord with a cleat at a Stop the Bleed course on 14 Mar 2026. I’m not one to be sold on an idea without thoroughly testing it out. After practicing with them since, I’ve become a believer in the Rapid Application Tourniquet System, alternatively known as the RAPID tourniquet, or the RATS.
Stop the Bleed instructors teaching a CERT, Community Emergency Response Team (a post-9/11 FEMA program), Googling how to use a RATS, the first time we played with one. Both of these experienced coaches have used other tourniquets in the field to stop real bleeding. The one on the left has also been stabbed.
As I said, wider is better. My friend and fellow ICSAVE instructor Ken S. is a paramedic on life flight helicopters. He once rolled up on a motorcycle accident, a partial amputation that a well-meaning bystander had turned into a complete amputation by using a boot lace to “tourniquet” it.
Ken teaching nursing students how to use tourniquets (in this case, CATs)
Tourniquets should be at least an inch wide, preferably two or more. Think trying to pinch a garden hose against the ground with the sole of your shoe, rather than with a fingertip.
At first glance, the RATS looks too thin to be an effective tourniquet. Plus, there’s that big metal cleat that looks like it’d dig deeply into the patient’s flesh.
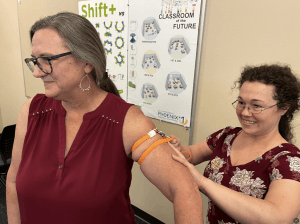
This school nurse did not appear to be bothered by the cleat. Any tourniquet, properly applied, will stretch and perhaps even fold your flesh a bit.
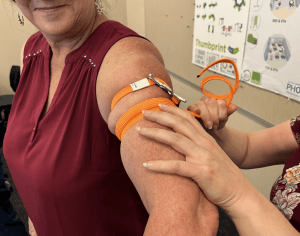
To solve the width issue, the key is to “widen” it with spiral, adjacent (not overlapping) wraps.
Do not stack the current wrap on top of the last, but rather, lay it down next to the previous. Try not to get the wraps too far apart. I’d be concerned about compartment syndrome if the wraps are separated by several inches, even though the wraps are spiral.
Wraps 2 & 3 are closer together here; wraps 1 and two, not so muchThis is textbook “adjacent but not overlapping” with a RATS. Some overlap must occur when you bring the loose, working end back across your wraps to lock it into the cleat.
More wraps is better. The goal is to make the overall coverage 1.5 to 3 inches wide. I couldn’t quite get three wraps around my upper leg, at first. With effort (and perhaps the practice RATS breaking in a bit) I was able to get three.
Two wraps around my thick leg was all I could manage over my sweats at first
With a friend, I was able to get 4 wraps or so around her much slimmer leg, even over her baggy pyjama-type pants.
I found the RATS easy to teach to others. Once they figure out how to run the rabbit (the free end of the bungee) through the hole (the three finger-wide triangle by the cleat) and reverse direction to establish a “trucker’s hitch,” the rest is intuitive.
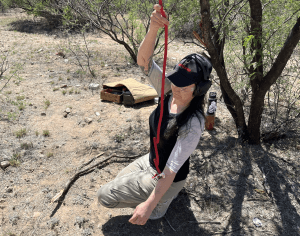
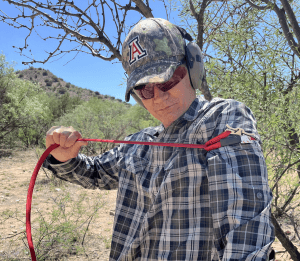
To get a RAPID started one-handed, let it unwind by hanging it from the the loose / working end. Drape the end with the cleat over your injured arm, with the cleat toward your front.Run the loose end around the back and underneath your arm, then run it through the triangle (Rapid Medical calls that triangle the “3 finger loop”).Cinch the resulting “trucker’s hitch” back the other way and start wrapping.
Hooking the free end into the cleat is dirt simple.
“Finishing” a RATS is much simpler than finishing CAT application. Simply hook the loose working end in the cleat and cinch back into it.
*****
Do You Need a Knot?
Some have suggested tying a knot above the cleat, to make sure it doesn’t work loose, but I don’t believe that’s necessary. I saw that “need for a knot shortcoming” on an internet post that may have been “guerrilla marketing” by a competitor. The instructions that come with the RATS, or on the Rapid Medical website, say nothing about tying a knot.
Unless you will be beyond help for several days, you would NOT ever loosen a tourniquet you put on a limb that is really bleeding. But when we practice, we put them on and take them off shortly thereafter. Sometimes in practice, we have a hard time pulling the loose, working end OUT of the cleat once we’re done applying it. I don’t think the “knot necessity” is a real thing.
*****
Keep it Tight
The hardest part of RATS application to master is pulling the bungee tight, and keeping it tight, as you apply it.
As with turning the windlass on more conventional tourniquets, students tend to not pull the bungee material tight enough without coaching. “Well, of course in the real thing I would pull it tighter, but I don’t want to hurt them,” is the typical rationalization.
This student did very well on her first attempt with a RATS, but like most, had to be encouraged to pull the RAPID tourniquet tighter.
But this is true:
Yea, verily, as ye train, even thus shall ye fight.
More often than not, when you are under life or death pressure, you subconsciously do it EXACTLY the way you trained, even if you don’t intend to, or even if the way you trained was only half of what it should have been.
Put differently, in the wisdom of Front Sight Rangemaster Moon:
“If you practice crappy technique, all you will become is a crap master.”
Why so Tight?
It bears mention here that a snug but not tight tourniquet will kill your patient faster than no tourniquet at all.
As with the restricting band they used on you when you last gave blood at the doctor’s office or Red Cross blood bank, the arteries can force blood into the limb past a snug (but not tight) tourniquet, but the snugness will restrict return to the heart though the non-pressurized veins. The blood will back up in the vessels and seek the path of lesser resistance–out through the hole that is causing the bleed.
In other words, if you put a tourniquet on snug, but not tight, ’cause you don’t want to hurt your patient, congratulations: you just made them bleed out faster.
Tourniquets need to be TIGHT–so tight, it feels like you are pinching the limb off. With a windlass-tightened tourniquet, the instructions are to tighten it till the bleeding stops, but in reality if the patient’s limb moves (changing the shape of the internal musculature) or if the tourniquet gets shifted during transport, the bleeding can start again if you only go that far.
When a tourniquet is tight enough, the fitness device should read __ beats per minute, like this one
Tighten a windlass at least a half a turn past when the bleeding stops. Like nuking Aliens from orbit, it’s the only way to be sure.
*****
How do we teach people to apply tourniquets tightly?
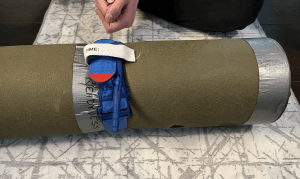
You can use a fake leg, like a thick pool noodle or a rolled up sleeping mat, for something to wrap a training tourniquet around. Students will not be afraid to hurt it, so they will be less reluctant to tighten the tourniquet adequately.
Training aid, courtesy of Crosswalk Readiness
But that still leaves them reluctant to “hurt” a real patient by applying a lifesaving device properly.
*****
It’s OK, You Won’t Break Me
We prefer to use real humans as tourniquet training “manikins,” for several reasons:
A real tourniquet will pull the skin and bend the flesh around it. Students need to anticipate that and know that it’s OK.
There is no manikin more realistic than a real human. Some skills cannot be practiced on a real living uninjured human. Cutting off the limb of a casualty pinned under a crashed helicopter in an active combat zone cannot be practiced on living role players (use cadavers or manikins instead). Nor can we do chest compressions or full-force abdominal thrusts or practice appendectomy.
Practice placing tourniquets tightly on real people without detrimental effect reinforces the notion that they will not harm the patient nor cause lasting damage.
Knowing patients can handle the pain makes caregivers less reluctant to cause them pain by properly tightening a tourniquet.
Knowing YOU can handle the pain of a properly applied tourniquet, when you are being the “manikin” for your training partner, inures you to the pain. In the real thing you will have less reluctance to tighten it adequately on yourself, and you will have less anxiety in an already anxious situation. Less fear and anxiety will make your blood pressure lower. Lower BP means you will not bleed out as fast before the tourniquet completely locks it down.
“If you’re not bruised 2 days later, did you even try?” asked this tough-as-nails educator who tried out the RATS
*****
Smaller Diameter Arms
One huge downside of the CAT is the flat plastic plate that the mounts the windlass and windlass clip. The plate only bends so far and doesn’t really work with smaller diameter arms like those of a child or K9. The cross-section of a child’s arm with a CAT applied looks like a D, with two corners, rather than an O.
In contrast, the SWAT (Stretch, Wrap, And Tuck tourniquet–a glorified exercise band) and the RATS have all the corners of an oval, so they work better on smaller limbs. Properly applied, even the soft, stretchy SWAT smarts a bit.
The Stretch, Wrap, And Tuck (SWAT) tourniquet
The reversing direction of the “trucker’s hitch” of a RAPID tourniquet makes it easier to start out putting on yourself one handed than a SWAT.
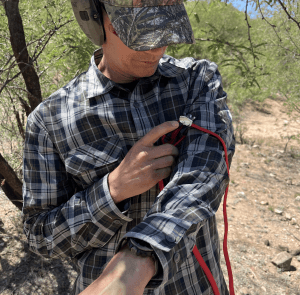
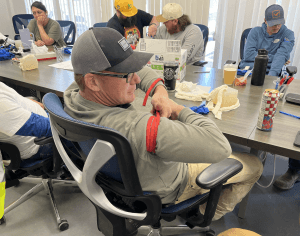
But another downside I’ve found of the RAPID tourniquet, so far, is that putting it on one handed requires some assistance from the wounded arm. In order to keep the tension up, when you’re putting it on your opposite arm one handed, one must be able to bend the arm that’s getting the tourniquet as you work your way around the arm with your good hand.
These wraps are way too far apart, which can be solved with training (it was his first time). What can’t be solved with training is that the arm you are applying it to could possibly be like a wet noodle.
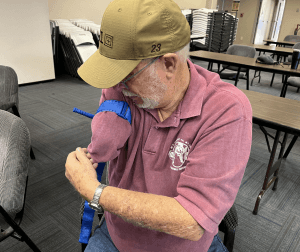
Of course, you won’t have to worry about the wounded forearm getting in the way if you are tourniqueting a complete amputation, as this legendary Southern Arizona lawman is practicing.
*****
Less Cube for EDC
When I was an AECM (aeromedical evacuation crew member) on C-130s, our Hercs would “cube-out” before they “grossed-out.”
187 Aeromedical Evac Squadron mates Stormy C and Bill N after marshaling one of our Hercs
In other words, we could almost always haul more tonnage than we had on board. We ran out of cubic space to stuff things in the bird before we exceeded our gross takeoff weight.
The RATS doesn’t take up much space and can easily be part of your EDC, every day carry.
Relative cube, L to R: CAT, RATS, TMT in package, and SWAT. ALWAYS REMOVE YOUR TOURNIQUET FROM ITS SHRINK-WRAPPED PACKAGE AS SOON AS YOU GET IT! You don’t want to be trying to pry that out of there, one handed, with sweaty or bloody fingers.
I eat enough doughnuts that my belt has plenty of room for a CAT, affixed with a pair of belt keepers. I have a large enough panza that shirts hang in front of it and it doesn’t “print.” Those of you who are fitter may want to carry a smaller tourniquet.
The velcro on the CAT does pick up some lint.
As with other tourniquets, you should remove a RATS from its wrapper as soon as you get it. Don’t wait till after you are down to one hand and those fingers are slippery with sweat and / or blood.
*****
Cost
I’m reluctant to list price points, because they change, but right now the RATS goes for about $25 each. I ordered a 5-pack of RAPIDs from the manufacturer for less than $100 before tax and shipping.
In 2025 I taught some Care Under Fire classes for television crews from the United Kingdom who were in the ‘States to ride along with Pima County deputies. Their IFAKs had TMTs, Tactical Mechanical Tourniquets.
The TMT, with its distinctive locking windlass clip
I bought a few TMTs as trainers so the TV crews could keep their “go-to” tourniquets pristine, saving them for the real deal. You, too, should practice with and wear out a dedicated training version of your go-to, rather than your go-to tourniquet.
TV crew using knee pressure on femoral pressure points to slow simulated bleeding while applying dedicated training TMTs to the role-playing patient.
Those TMTs cost me 31.69 each before shipping.
CATs, by means of comparison, retail for around $39. You might find a better price, but regardless of the tourniquet you choose, be sure it is the real deal, not some cheap knock off that will break when you try to use it. The best way to do that is to order directly from the manufacturer.
The CAT is made by North American Rescue.
The SWAT-T is made by H&H Medical, a division of Safeguard Medical.
The RATS is made by Rapid Medical (RapidTQ.com).
The SOFTT-W is made by TacMed Solutions.
The TMT is by Safeguard Medical.
Disclosing: Nothing to Disclose
I have ZERO fiduciary interest in Rapid Medical, North American Rescue, TacMed Solutions, H&H Medical, Safeguard Medical, nor any other company that sells medical equipment. If I tell you a piece of gear works well, or doesn’t work well, it’s because, as far as I can tell (see Should be Taken with Salt below), it works well, or it does not.
You can take that to the hospital–alive.
*****
CoTCCC vs FDA
There are numerous makes and models of effective tourniquets out there, and some pieces of junk, too. For example, the Seraket Universal Automatic “Tourniquet” is NOT a tourniquet, regardless of its name. The Seraket is a restricting band, great for blood draws but not useful at all to stop exsanguinating hemorrhage.
The Committee on Tactical Combat Casualty Care (CoTCCC, or “COT-see”) periodically reviews tourniquets. The most recent update of the CoTCCC guidelines I’ve found does NOT have the RATS on their list of “recommended” tourniquets. CoTCCC found that the RATS takes longer than, say, a CAT, before you have enough wraps to slow the bleeding significantly.
My experience with the RATS, thus far, has mimicked CoTCCC’s: applying a RAPID, it takes several seconds longer than that “first pull” on a CAT before you have enough wraps to start feeling a difference in circulation to the limb.
Properly applied, a CAT should start to restrict blood flow to the limb before one even starts to wind the windlass. With training, and a properly pre-staged CAT, that can be done in only a few seconds.
It should be noted, though, that although CoTCCC reviews literature to advise on whether a given piece of equipment or protocol is apropos under rigorous combat conditions, they do not have a regular submission and review process for new products that I am aware of. They do not review every tourniquet, and they do not continually evaluate what’s out there. They do so from time to time.
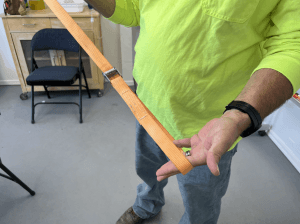
A student who works outdoors told me he carries this locking cinch-strap on him to use as a de-facto tourniquet if he needs one in the wilderness. It is light and doesn’t take up much cube. He is ahead of the game from even thinking he might need something like that, and carrying it on him religiously. But this has not been tested by any certifying medical agency I am aware of. I had him try it out on me, and he could get it little tighter than a restricting band. Better than nothing? Sure. Would I bet my life on it, if I could afford a CAT or a RATS instead? Probably not.
Further, CoTCCC is not a regulatory body, and does not “approve” anything (although the phrase “CoTCCC approved” appears frequently in advertising and on internet forums). In the US, the Food and Drug Administration (FDA) approves equipment for medical practice.
From what I’ve been able to glean, the RATS is registered with the FDA and therefore approved for sale in the US. The FDA has not, to my knowledge, issued any sort of report or guideline evaluating the efficacy of the RATS.
Neither Heloderm nor ICSAVE is in the habit of endorsing any given piece of gear. Instead, we seek to give our students options and information they can use to make informed decisions for themselves.
Newer is not necessarily better, but in this case, it is. I would avoid using these antique tourniquet designs, although the wide elastic strap on the bottom might work if pulled and secured tightly enough.
I still prefer the CAT for most adult applications. I’ve added the RATS to the SWAT-T when teaching educators, veterinarians, school nurses, and preschool personnel who deal with populations that have narrow-diameter limbs.
InterVol / ICSAVE students in a formation I call a “Lima wheel” (because their legs are like spokes and I learned this instructional technique from a BorSTAR agent named Lima) place tourniquets on the left leg of the person to their right. Most are practicing with CATs, but the woman in the denim shirt is putting a SWAT on the boy in the KRAKEN shirt.
*****
Should be Taken with Salt
This report, like a lot of the fluff available on the internet, is long on conjecture but short on real-world experience.
I’m a NAEMT certified TCCC and TECC instructor. I taught 1,200+ people to use tourniquets in 2025. Conservatively, that extrapolates to 10,000+ I’ve taught to control bleeding over the last several years. Several of our students (that we know of) have used tourniquets to stop exsanguinating hemorrhage (bleeding out). But I have never, ever, used a RATS to save a life.
So think for yourself and do your research before you invest your department’s entire IFAK budget for the next fiscal year into RAPID tourniquets.
The Mechanical Advantage Tourniquet (MAT) was the only tourniquet my agency’s TacMed program director authorized us to use when serving warrants–til we figured out that bumping the red button or something accidentally hooking under the tab on that buckle would loosen it, killing the patient. A tourniquet needs a quick release button like a fish needs a bicycle, and a woman needs a man. Pyng Medical now makes an upgraded version of the MAT, but I don’t know if they’ve removed the dangerous and unnecessary quick release button.
*****
Appendix:
Not Till I Tell You
There are several anecdotal accounts of severely wounded soldiers and police officers who started to lose consciousness before hearing, in the back of their minds, echoes of their DIs or Academy Instructors yelling at them, “On your feet! You’re not dead till I tell you you’re dead!” They rallied long enough to solve the problem and survived to tell the tale.
As with other tourniquets, I found that the pain of a RAPID tightly wrapped around my leg did not prevent me from demonstrating that just ’cause you have a tourniquet on does NOT mean you’re down for the count. You can run, walk, crawl, and carry or drag others to safety.
There’s a RAPID on the left leg; it hasn’t incapacitated this rescuer
Moving after applying a tourniquet is a standard part of our training. That way, our students will not have to wonder. They will know that they will not be helpless if they have been shot in a limb and have a tourniquet applied. They can still run or fight if the bad guy comes back to finish the job.
This adolescent can not only handle the pain of a properly applied tourniquet, she can still save herself and others. Can you?